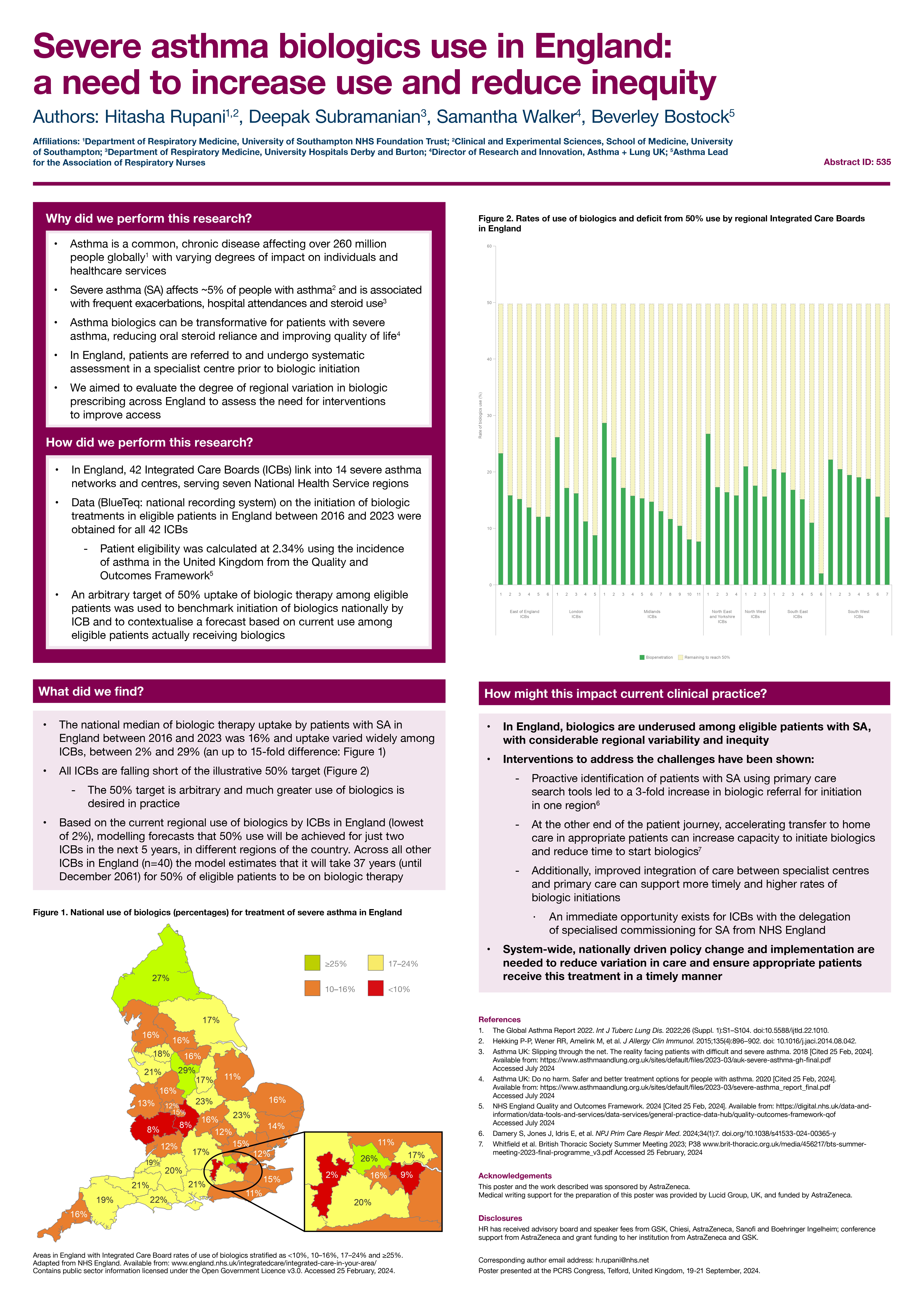
Severe asthma biologics use in England: a need to increase use and reduce inequity (ID 535)
University Hospital Southampton NHS Foundation Trust
This abstract has been submitted to ERS and BTS, therefore under embargo and cannot be published at acceptance, until we hear notification of BTS.
Funding: This abstract was funded by AstraZeneca
Conflicts of interest: Hitasha Rupani has received advisory board and speaker fees from GSK, Chiesi, AstraZeneca, Sanofi and Boehringer Ingelheim; conference support from AstraZeneca and grant funding to her institution from AstraZeneca and GSK.