A Service Evaluation following the implementation of Computer Guided Consultation Software to support Primary Care Reviews for Chronic Obstructive Pulmonary Disease (ID 494)
Liverpool University Hospitals NHS Foundation Trust
Abstract
Objectives: This study evaluates a digital solution aiming to support Chronic Obstructive Pulmonary Disease (COPD) reviews, focusing on the impact of implementing guideline-standard care using Clinical Decision Support System software in the form of a computer-guided consultation (CGC).
Methods and Analysis: The CGC is an intelligent decision support system enabling accurate diagnosis of COPD and prompts holistic guideline-standard pharmacological and non-pharmacological management. Patients on primary care COPD registers across 254 general practices nationwide were identified through a structured clinical pathway and subsequently underwent review using the CGC linked directly to the primary care clinical system.
Results: 5,221 patients on the COPD register were reviewed and of those, 21.1% were found not to have COPD following CGC review. When considering those with an established diagnosis of COPD following CGC review, the CGC highlighted findings of previously unrecognised new onset cardiac disease in 7%. CGC review resulted in the number of patients possessing a written management plan rising from 62% to 85% (McNemar’s test; p<0.001). 28% of the cohort were current smokers, of whom 99% were counselled regarding smoking cessation following CGC prompting. 13% were found to have sub-optimal inhaler technique during CGC review with the CGC prompting correction of deficient technique or other intervention in all cases. The CGC identified 1,996 patients deemed appropriate to be referred to Pulmonary Rehabilitation (PR) according to guidelines, of whom only 26% had previously attended a PR program. CGC review found that 11% and 10% of patients had not been up to date with Influenza and Pneumococcal Vaccination respectively.
Conclusion: The integration of technology in the form of clinical decision support system software within the clinical pathway described is more likely to result in an accurate diagnosis of COPD and greater implementation of guideline-level care representing a scalable solution when performing primary care COPD reviews.
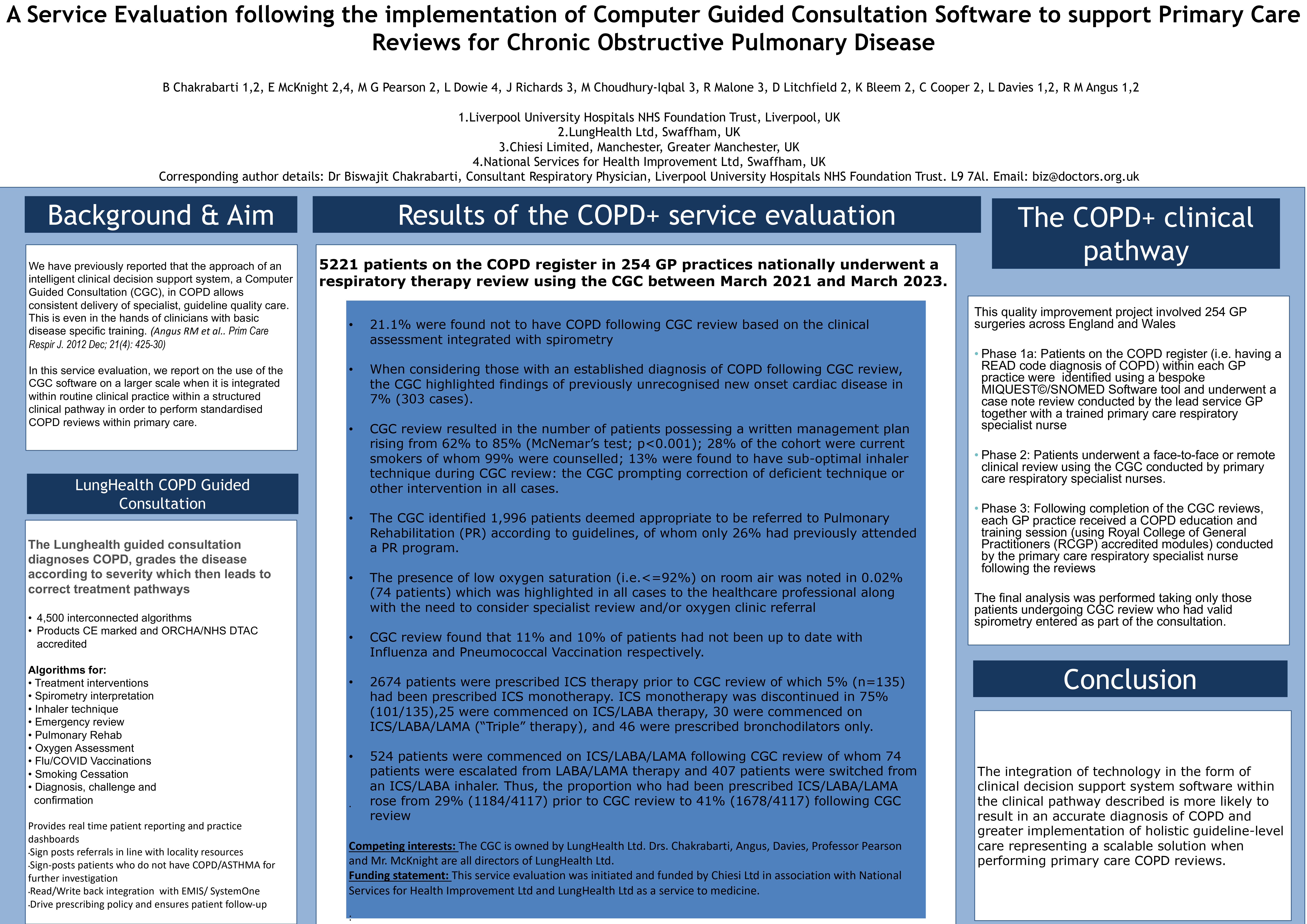
Funding: This service evaluation was initiated and funded by Chiesi Ltd in association with National Services for Health Improvement Ltd and LungHealth Ltd as a service to medicine.
Conflicts of interest: The CGC was created and programmed by Biswajit Chakrabarti, Lisa Davies, Robert Angus, Michael Pearson, Kash Bleem, Chris Cooper, David Litchfield, Mark Osborne, Eddie McKnight and Louise Dowie, and is owned by LungHealth Ltd. Drs. Chakrabarti, Angus, Davies, Professor Pearson and Mr. McKnight are all directors of LungHealth Ltd.